



Study characteristics
A total of 31 studies were included, with pregnant women from diverse ethnic backgrounds, socioeconomic statuses, and age groups represented. The characteristics of the included studies can be found in Table 1.
Qualitative studies included in the review were conducted in Canada [17, 18], Iran [19, 20], China [21], Germany [22], Nepal [23], Australia [24,25,26,27], Brazil [28] and the United States of America [29, 30], with a total of 14 studies. These studies involved methods such as focus group discussions [18, 19, 22, 25, 29, 30], face-to-face and [19,20,21,22, 26,27,28] telephone [17, 24, 27] in-depth interviews to explore pregnant women’s perceptions, attitudes, and experiences regarding oral health care.
A total of 16 quantitative, cross-sectional studies, were conducted across Canada [31], Saudi Arabia [32], Colombia [33], India [34], Australia [35, 36], Pakistan [37, 38], the United States of America [39,40,41,42,43], Iraq [44], Nepal [45], and Thailand [46]. These studies utilized surveys to gather data on factors influencing dental service utilization, dental anxiety, knowledge, attitudes, and practices related to oral health during pregnancy. Analytical approaches included statistical tests.
Furthermore, a clinical trial study [47] conducted in Iran involved 110 pregnant women (55 in the experimental group and 55 in the control group), where there was a teaching intervention session. Data collection was carried out using a questionnaire based on the Health Belief Model (HBM), focusing on oral and dental hygiene behaviours in pregnant women.
Risk of bias within studies
Using the Mixed Methods Appraisal Tool (MMAT), as displayed in Table 2, all studies were found to have clear research questions and appropriate data collection methods. The qualitative approach and data collection methods used were deemed adequate, and the findings were comprehensive, coherent, and well-supported by data. The study by Maybury et al. 2019 [40] was considered a qualitative and cross-sectional study.
The Newcastle-Ottawa quality assessment scale, adapted for cross-sectional studies. showed the risk of bias analysis and quality assessment of the included studies and the results are displayed in Table 3. The scores varied from high [34, 37, 38, 40, 44,45,46], medium [31,32,33, 35, 36, 41,42,43] and low [39] risk of bias in the fifteen studies. The majority of the studies presented a moderate or high risk of bias.
SELECTION: Representativeness of the cases, Sample size, non-response rate, Ascertainment of the exposure (risk factor); COMPARABILITY: The potential confounders were investigated*; OUTCOME: Assessment of Outcome, Statistical test. Scores, 0–4: high risk of bias; 5–7: medium risk of bias; 8–10: low risk of bias.
*In the “Comparability” section, a new option of 0 score was added when the study did not investigate potential cofounders.
Results of individual studies
In this systematic review, we examined 31 studies to identify barriers to accessing oral healthcare during pregnancy. The included studies revealed several barriers pregnant women face when seeking dental care. The barriers identified are presented in Fig. 3.

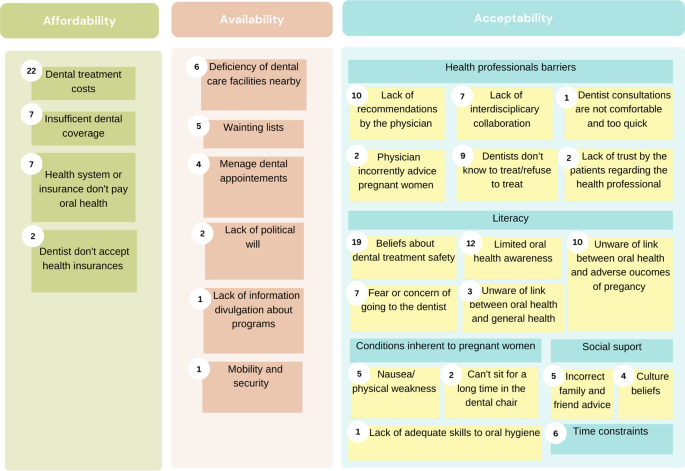
Results summary: Illustration of the barriers identified across included studies
This figure summarizes the findings from the 31 included articles, focusing on three dimensions: affordability, availability, and acceptability. Each small rectangle represents a specific barrier identified in the review, with the number next to it indicating how many articles mentioned that particular barrier.
Affordability emerged as a major concern, with 22 out of 31 studies [17,18,19, 23,24,25,26,27, 31, 33, 34, 36,37,38,39,40,41,42,43,44,45, 47] highlighting the significant impact of dental treatment costs. Additionally, 7 studies [17,18,19,20, 26, 27, 34] noted barriers related to insufficient dental coverage and health systems or insurance not covering oral health expenses [19, 26, 39,40,41,42,43].
Availability barriers were also prevalent, with 6 studies [18, 23, 25, 31, 38, 39, 44] reporting deficiencies in dental care facilities, while waiting lists and difficulty managing dental appointments were mentioned in 5 [21, 25, 27, 31, 40] and 4 studies [21, 27, 35, 39], respectively.
Barriers to healthcare access during pregnancy include issues with healthcare professionals, literacy, and social support. Specifically, 10 studies [17, 19, 22, 29,30,31, 37, 38, 40, 45] highlighted the lack of recommendations by physicians and 6 studies emphasizing inadequate interdisciplinary collaboration [17, 19, 21, 25, 29, 44]. Dentists’ attitudes were also a concern, with 6 studies [19, 21, 29, 31, 41, 42] citing a lack of knowledge about dental appointments for pregnant women and even cases of treatment refusal. Lack of trust in healthcare professionals was also stated in 2 studies [35, 39]. Regarding literacy-related barriers, 19 studies [19,20,21, 23,24,25, 27, 30, 31, 34, 36, 37, 40,41,42,43, 45,46,47] refer to concerns about the safety of dental treatment, while 12 studies [17, 20,21,22, 26, 29, 31, 35, 36, 38, 40, 45] noted limited oral health awareness, unawareness of the association between oral health and pregnancy [18, 22, 25, 27,28,29,30, 35, 40, 46], and/or think oral health and general health are separated [17, 18, 30, 35]. Moreover, 8 studies [17, 18, 26,27,28, 32, 39, 44] highlighted fear or apprehension about dental visits.
Physical discomfort [19, 20, 22, 31], misguided advice from family and friends [18, 30, 31, 34, 45], cultural beliefs [19, 25, 27, 38], and time constraints [19, 21, 36, 37, 44, 45] were also identified as barriers across the studies.
link